This is just a short post about what Artificial Intelligence is in very basic terms, in subsequent posts I am going to go into more detail about the actual workings. But for now, I am just going to classify AI and discuss what might be needed to improve on what we already have.
First let’s define what AI is.
It stands for artificial intelligence, and in basic terms is the development of a computer system having the ability to perform tasks normally requiring human intelligence. These are tasks such as visual perception, speech recognition, decision making etc.
AI can also be described as an ‘intelligent agent’ which is any device that perceives its environment and takes action to maximise its success achieving its goals.
The essence of these systems is to acquire heuristic knowledge (that is facts and information) about a situation allowing it to then learn from this data, absorbing what aspects of the data will be correlated to others and thus it can then make predictions on sets of unknown data. This is really quite similar to the way that our own human brains learn to respond to the environment around us:
We take in data (e.g. this flickering red-orange thing is called fire)
We learn what it represents and what effect it has on the world (it is hot… do not touch)
When presented with similar data in the future we can predict the outcome without having to actually have the answer (don’t touch fire).
For us, this is clearly quite a simple process to wrap our heads around, but as children we spend those early years trying to learn from the environment, constantly making mistakes and refining our biological algorithms to improve our understanding of the world.
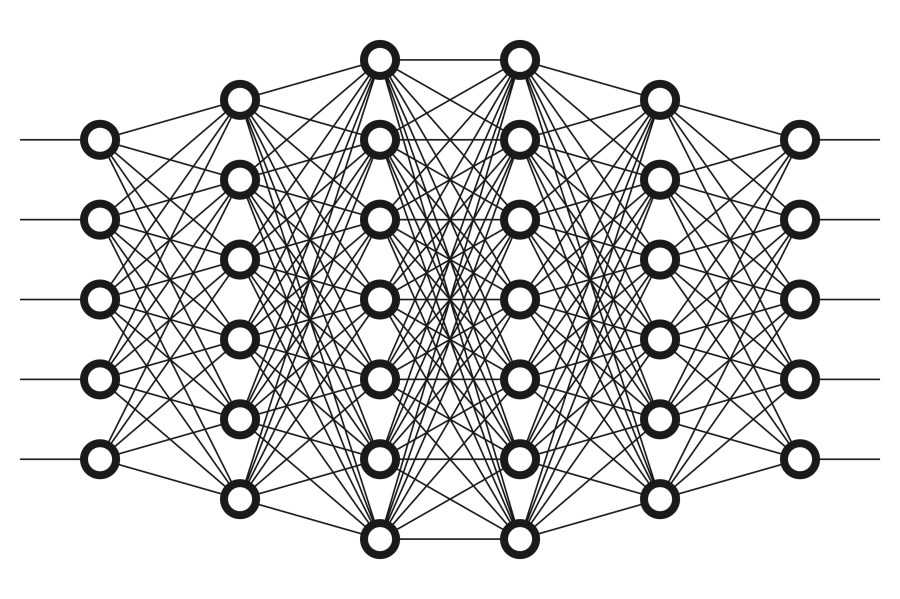
For machines these simple algorithms also wouldn’t be the hardest to compute either, but the problem arises when we try to create machines capable of learning from lots of different data and classifying it into its own network from which it can constantly expand and improve. A network very similar to our own brain. In fact, we only know that such an intelligence may be possible in machines because we ourselves are the embodiment of that vision. We have/are an example of a network of connecting processes that is able to interpret and learn from its environment, thus as some sort of intelligent agent.
It would only make sense to base these artificial intelligences on what we know works – the brain. This has sort of what has been done with the deep learning and machine learning that we current use.
The problem now is that the collaboration between the two fields of neuroscience and AI no longer communicate and learn from each other in a way that would be beneficial for the development of the technology, there seems to be a saddening disparity between the two fields, with each discipline having grown in complexity and thus further apart, coagulating their own boundaries between one another. Obviously there are differences between the two subjects and the practical aspects of building an AI system may not always adhere to biological guidelines, but learning from these (proven to work) guides probably can’t hurt (probably.)
So, currently we are at the stage where we are able to create a system which is specialised to have a very specific range of abilities. This is called narrow AI (or weak AI). A narrow AI may be pretty amazing at recognising objects such as the numbers 1-10, but if you show it a dog it will have no idea. It will confidently try to make a prediction but will most definitely be wrong (like when a child only knows four animals and therefore every animal it sees is bound to be one of these.)
Regardless of the narrowness of the current AI abilities, it is clear that it has accomplished some specialised application in a number of areas:
Perceiving its environment through “senses”
Learning and reasoning (e.g IBM’s Deep Blue Chess machine)
Natural Language Processing (NLP) for speech recognition or translation.
Controlling machines (such as drones or cars)
The goal in the future will be to improve this narrow AI to the point where a machine would be able to possess a number of these narrower forms of intelligence, perhaps with an increasingly wide range of goals in numerous diverse context (perhaps even beyond the average adult) this may classify as what is known as artificial general intelligence (AGI).
I think that’s enough to conclude on, I will at some point go into the actual workings of our current AI, but for now it’s clear that we have a long way to go to develop this kind of AGI that people think of from science fiction (like Skynet in terminator). I do think that this higher-level intelligence is possible it’s just about how we get there, and I think it really comes down to this collaboration between fields where neuroscientists/computer scientists can study this living specimen of higher intellect and try to transfer it in a machine.
I found it reasonably tricky to really know how to separate this post into what’s actually important. Alcohol to me is a weird substance both chemically and socially I suppose. The culture surrounding alcohol is very different all around the world, but speaking from the perspective of the UK, it is very unhealthy/binge related. There seems to be this idea that alcohol is not that dangerous, that perhaps the worst that can happen is just some embarrassing memories (or lack thereof) and is regaled as a sort of rite of passage to adult-hood but this is not true. I mean putting aside the chemical effects for a second, it seems crazy that we have socially formulated this idea and positively look forward to being old enough to legally liquidate our brains slowly and ritualistically. But anyway, that’s not really what this post is about. It’s mainly about 3 things. One, how does alcohol affect the brian from a bio-chemical perspective (mostly on neurotransmitters). Two, what (broad) effects does alcohol have on different brain regions (ie with short term usage). Three, the dangers of alcohol on the brain (I.e long term use and addiction).
Alcohols effects on neurotransmitters
Alcohol is a type of substance known as a central nervous system depressant (CNS Depressant), and can effect our brain chemistry primarily by altering the affects of neurotransmitters. Neurotransmitters can be either excitatory or inhibitory. Excitatory neurotransmitters stimulate brain activity, inhibitory neurotransmitters suppress it.
Alcohol works primarily in two ways: it increases the effects of the inhibitory neurotransmitter GABA and also inhibits the excitatory neurotransmitter Glutamate. As well as its role on GABA and Glutamate alcohol facilitates dopamine release and also acts on channels in the synaptic membrane, all of these effects can cause short term problems as well as long-term damage.
GABA
GABA (which stands for Gamma Aminobutyric Acid – but who would bother calling it that) is a neurotransmitter in the brain that decreases the activity in the nervous system, its natural function is to reduce the activity of the neurons it binds to by inhibiting/blocking their signal. It is believed GABA can generally reduce our fear/stress due to overexcited neurons. This is why it is the target of a lot of depressant drugs such as benzodiazepines (such as Valium and Xanax) and also where alcohol has its effect. By increasing the amount of GABA in the brain it may feel like a stress reliever and may act to kind of slow everything down; however, it also causes this sluggish movement, poor motor function and slurred speech associated with alcohol consumption.
Glutamate
Glutamate is a neurotransmitter that basically does the opposite it makes neurons excited, hence being called an excitatory neurotransmitter. It increases brain activity and is involved in many cognitive functions such as learning and memory. It also seems like the optimum balance of Glutamate is important as too much glutamate release leads to seizures and death of brain cells and too little glutamate leads to psychosis coma and death. What alcohol does is actually inhibit the amount of Glutamate released thus decreasing levels, supressing this stimulant results in a similar type of physiological slowdown as seen with GABA increase. It is therefore understandable why alcohol is regarded as a general depressant.
Dopamine
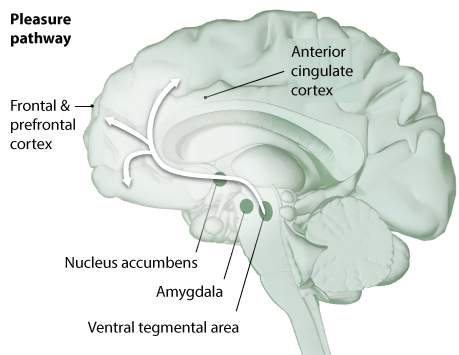
What alcohol also does (like many other drugs) is increase the amount of dopamine in the brain. Dopamine basically gives us the feeling of pleasure (particularly in the ventral striatum, including a pathway from the ventral tegmental area (VTA) though the nucleus accumbens and to the pre-frontal cortex (PFC) – not important for understanding is just a pathway that causes the feeling of pleasure). We (hopefully) feel pleasure a-lot of the time, and should happen during any “pleasurable activity”, from getting a promotion to seeing friends or gaming, gambling or taking crack. This feeling of pleasure that alcohol provides (when used frequently) is what causes so many to become addicted. Alcohol tells your brain that you feel great! You like feeling great and so continue to ply your brain with this feel-great-smoothie. Now your brain gets more and more used to being made to feel great every day that it gains a tolerance to this substance.
Diagram showing the “pleasure pathway” from VTA to PFC and the rest of the cortex.
Now it takes more alcohol than it used to, to make you feel as good. The brain has stopped producing as much natural dopamine because it’s used to just being given it daily. Now other things that used to give you pleasure, just aren’t as pleasurable and the only thing to satisfy that itch is alcohol. When you don’t drink you feel awful, and so you self-medicate with alcohol to feel okay again. This is why it’s so hard to get over an addiction, because you are no longer drinking to feel good, you are drinking to just feel normal.
(This idea of dopamine release is crucial to almost any addiction – if you want to learn more about how addiction works in more detail see here.)
Voltage Dependant Calcium Channels (VDCCs)
Alcohol can also work on channels in the presynaptic membrane called the voltage dependant calcium channels (VDCCs). VDCCs are used at the pre-synaptic neuron to facilitate the release of neurotransmitters across the synapse. Alcohol blocks these channels and stops calcium from being released.
Now if we look at this in terms of addiction, we saw that when the brain was pumped with a dopamine releasing substance it couldn’t release as much without it. The same sort of thing happens here. The neuron can’t release calcium because the channels are blocked, so it makes more channels so that calcium can still be released (this provides tolerance to the drug – then you drink more). This process repeats until there is a huge excess of VDCCs (most of which are blocked) to release the required calcium into the neuron.
Now let’s imagine that you stop drinking suddenly, these VDCCs will no longer be blocked and there will be a huge influx (entry) of calcium into the neuron. The neuron will be flooded with way more calcium than it needs and this calcium will cause too much release of neurotransmitter to activate other neurons. Neurons that were usually just about stimulated into action are now completely overexcited and can lead to withdrawal symptoms like: Tremor, nausea, fever, sweating, hallucinations and sometimes seizures. It seems quite clear how these symptoms are cause, if alcohol normally depresses our brain activity and increases the mechanisms (like calcium release) to be able to function normally. When you remove the alcohol the brain activity will be overloaded thus causing these symptoms associated with overstimulation.
Regions of the Brain that Alcohol affects
Now that we have looked at how alcohol affects the biochemistry of the brain, let’s move onto some of the regions of the brain that alcohol actually acts on each time you drink and what effects this will have in the short term. after-this we will look at the permanent effects drinking has when it is done frequently.
Just a visual reference, here is a brain. the only labels we need to worry about are the frontal lobe, hippocampus, amygdala, cerebellum and medulla (which is in the brainstem)
Frontal Lobes
Let’s start with some mild drinking, you have a pint maybe some wine and you feel a bit giggly, you start to feel the stress ebb away, and so it begins. Alcohol will start to general impair many functions of the frontal lobes which are in control of processes such as memory, cognition and judgement. So even information from our sensory receptors such as eyes and ears are slowed down, just slowly shutting off our understanding of what is going on around us. The frontal lobes also contain the prefrontal cortex (PFC). The PFC is an area of the brain that is highly developed in higher primates such as humans, it’s an area of our brain that is involved in a wide variety of executive function. It takes inputs from many regions of the brain and then adapts according to the inputs, making a final decision on what to do.
A part of this function is called inhibitory control. This is a cognitive process that permits an individual to inhibit their natural impulses or behavioural responses (prepontent responses). Essentially, it’s a function of the brain that allows us to say no. For example: You are presented with a rewarding stimulus – like some chocolate or some shots or whatever floats your boat. Without inhibition, a person might have an automatic response to just take it. The inhibitory controls allow us to evaluate this decision with regard to other functions like internal plans or general awareness (such as a diet or work the next day) and will then allow us to inhibit this response.
What alcohol does is actually depress this inhibitory response, making a person less inhibited. This means that a person is more likely to engage in foolishness without being able to inhibit their behaviours acceptable. You don’t need neuroscience to visualise this depression of inhibitory control. Alcohol makes a normally cautious and shy person turn into a table dancing, cone stealing, MacDonald’s eating, loud-mouth, who will more than likely stagger across roads without looking. This also means that once you have had your first drink it will probably make it harder and harder to say no to the subsequent rounds.
Cerebellum
Now you have had a couple of drinks, started to let go and loose some inhibition. Next the Alcohol will affect the Cerebellum which is involved with movement and coordination. The cerebellum is the little area at the back of the brain (literally translated from Latin as “little brain”) even though the cerebellum is quite small it consists of a number of subdivisions controlling or facilitating different behavioural functions. One of these areas called the Vermis (named so because of its worm-like appearance) the vermis is involved with movement and balance and are especially useful in the refinement of coordination. At this level of moderate alcohol consumption you will be feeling some postural instability maybe the characteristic staggering and will have some general incoordination.
Hypothalamus and Amygdala
Now you have had quite a few drinks, you came out for one drink but now you are six G&Ts down (and maybe some shots but you can’t remember) you’ve danced and fallen over and smoked a cigarette (even though you said you wouldn’t). The alcohol is now affecting other areas that relate to emotional response such as the hypothalamus and amygdala. You are now more likely to misinterpret people, maybe have a-little cry, perhaps fight that man in the street because he looked at you funny, you have turned from happy tipsy to angry drunk.
The amygdala is an interesting area buried deep within our brain that specialise in the linking of emotions to memories. The amygdala is responsible for the perceptions of emotions such as anger and sadness as well as regulation of aggression. It allows us to combine feelings with rational thought or experiences, so that we can be better prepared the next time. It allows us to be nervous in situations that might harm us and feel positive in good situations. It can also go wrong leaving us fearful of things we shouldn’t be that really don’t make sense, like clowns or the dark or autism from vaccines. Alcohol seems to inhibit the ability of the amygdala to attach the right feelings to situations. There is also evidence suggesting that alcohol inhibits the ability in heavy drinkers to process emotional faces, this may be due to the coupling between the amygdala and the orbito-frontal cortex.
The hypothalamus (and pituitary) control automatic brain functions and hormone release. A consequence of alcohol consumption on this is how it depresses nerve function in the hypothalamus that control sexual arousal and performance. So ironically sexual urge may increase, sexual performance will most certainly decrease.
Medulla
Now we have reached some heavy levels of drinking, you have drunk more alcohol than you ever thought was possible. At this point you are probably even beyond conscious thought. The alcohol is impairing the function of the medulla oblongata. This section of the brainstem controls basic vital life functions such as breathing, consciousness and heart rate. You have now reached “we should probably put you in an Uber, actually no, call an ambulance” level of drunk where you can ruminate on the mistake of drinking while they pump out your stomach. Alcohols depressant effects on the medulla is often responsible for the fatal signs of overdose such as respiratory depressionand slowed heartbeat. This requires quite a substantial amount of drinking in one sitting (well for most people) and can lead to this blackout level of drunk. (so in all seriousness if someone is this drunk and they don’t even respond, then do call an ambulance – and don’t let them sleep on their back. equally just don’t drink that much).
Its true alcohol does make you younger! Unfortunately, not by making you look any younger… Instead it slowly deadens your brains capabilities until you reach the state where the bodies just playing Russian-roulette for which basic brain function it can remove but still keep you alive. In a competition with a new-born child for who can balance on their feet and formulate basic sounds, I would put my money on the child. I mean the fact that the vast majority of the UK population consumes a substance like this so frequently that one of the hallmarks of our society is the crucial existence and age-old tradition of going to the pub is baffling. Its probably never going to change, something so engrained in our way of life have always proven hard to remove. Brits occupy pubs in the same way Americans occupy coffee shops.
Long-term damage caused by alcohol
We have looked at how alcohol will affect different brain regions and cause behavioural abnormalities in just a single sitting, but now let’s move on to some long term uses. Its now not just one or two pints per week, its more than 14 units per week on a recurring basis, alcohol has become a part of your routine. How does this continued usage damage the brain? and is there any way to reverse to process?
The first damaging aspect of long term usage that we have already mentioned above, is addiction. Too much of a good thing will cause some sort of addiction. We have seen above how addiction may be facilitated with induced dopamine release and calcium channel blockage (thus creating tolerance and withdrawal effects) and alcohol is definitely up there a dangerous addiction. Along side this aspect of addiction in craving the release of dopamine is the negative emotional effects it has on the rest of the brain such as depression and anxiety.
Alcohol will also generally cause breakdown (atrophy) of the brain cells where it is known to act (such as in the cerebellum, amygdala and frontal cortexes etc). Slowly alcohol will decrease the number of cells in certain regions of the brain inhibiting its natural ability to complete certain functions.
Atrophy in areas of the brain involved in memory can lead to mild deficits but can also develop into more serious conditions such as Wernicke-Korsakoff syndrome (WKS). WKS exists in two parts: A short-lived condition called Wernicke’s encephalopathy and the longer lasting Korsakoff’s psychosis. Wernicke’s encephalopathy results in symptoms such as mental confusion, paralysis of nerves that move the eyes, and difficulty with muscle coordination. About 80-90% of those with Wernicke’s will go on to develop Korsakoff’s psychosis which is a syndrome characterised by persistent learning and memory problems, the most prominent memory loss is with anterograde amnesia where people will struggle to lay down new information.
Further atrophy in areas of the brain such as the cerebellum is common in alcoholics, such as volume loss in the vermis which will lead to problems such as stance imbalance (known as gait ataxia) and coordination problems (such as motor control of hands and problems with vision). There is also a role for the cerebellar in language production and mental imagery formation which long term alcohol use may affect.
Conclusion
I feel like this is just a glimpse of the effects that alcohol can have on our brain from its effects on neurotransmitters and protein channels to its long term atrophy of important brain regions relating to memory, emotions, coordination and basic vital functions. Alcohol probably isn’t the worst thing (in moderation) but cant that be said for all drugs? if you were able to take heroin just once you wouldn’t face permanent damage, but it’s hard to take just once because of its addictive nature. Alcohol is no different, and is still addictive, if anything it’s perhaps even harder to resist because it is legal and used so widely in our society. It is clear that it defiantly has some pretty severe effects in both the short term and long term when abused yet as a population we continue to abuse it from about the ages of 18 until death, with about 80% of people drinking every year. Yes there are limits to when we can drink (such as driving or at work), and yes not everyone drinks in such high quantity that its necessarily dangerous, but I think we don’t appreciate the dangers of alcohol even in mild/moderate long term usage, we don’t know how much is too much, with many thinking they are not addicted (or dependant) even though they are drinking more than what would be classed as too much. Probably because it’s so normalised. To clarify – low risk alcohol consumption is classed as a maximum of 14 units per week (thats about 6 pints) with the recommendation being to spread out the units over the course of the week, and thats low risk not no risk. there are likely a vast percentage of the population who are exceeding this low-risk limit without even realising that they may have a problem. On top of this I have only been speaking about the dangers of alcohol to the brain, alcohol has so many other areas that it causes severe damage to (like liver, cardiovascular system, skin, increased risk of cancer and stroke and so much more). This post isn’t about scaring people into stopping drinking, its just giving an overview of effects and if that scares you then so be it…
The nervous system is responsible for receiving and processing all the information in the body. It is divided into two distinct sections, the central nervous system (CNS) which is comprised of the brain and spinal cord, and the peripheral nervous system (PNS) which is comprised of all our sensory organs and the nerves that connect them to the CNS. Though the structural formation of the nervous system is similar between people, they are also very unique, for the way that we as people are seems to be very much based around the slight differences in these structures.
How does the nervous system communicate?
The Nervous system is made up of two basic cells, The Neuron that transmit the message and the Glial cells that support them. The basic ‘design’ of a neuron is alike; however, like most cells in the body, neurons will be specialised to their specific role.
The neuron can be split into 3 parts: the antennae like fibrils called dendrites, the cell body which is where the nucleus of the neuron is and is used to provide energy to drive the neuronal activities, and the axon which is a long tail like structure that conducts an electrical signal to the other neurons (or whatever organ they innervate).
Now the basic way that the nervous system works is that the sensory receptors in say the eye perceive something (such as a ball flying toward you). The sensory receptor will send a signal (called an impulse) through its sensory neuron, the impulse will travel down its axon, that may then pass onto another neuron (through the dendrites, cell body and then down the axon of this neuron) until at some point it will reach the brain (in the case of the eye this will be to the visual cortex) where the brain will interpret what it sees. This impulse doesn’t just stay in the visual cortex but will be transmitted to other parts of the brain where it is interpreted and a decision is made about, what this input is, whether something needs to be done about it, and how can this be carried out. If it is decided that something does indeed need to be done, the brain will send an impulse down a motor neuron to the arm and the hand and the fingers to innervate whatever action it has designated (hopefully the catching of the ball.)
Alongside the sensory and motor neurons are the interneurons, these interneurons are the most common type of neuron and can pass signals directly from the sensory neuron to the motor neuron. They can form complex circuits that help us react to external stimuli. An example of interneurons in action is if you touch something hot. The sensory neurons in the finger send a signal to the interneurons in the spine, which will then relay some signals straight back into motor neurons in your hand causing them to move. Other signals will be relayed from the interneurons to the pain centres of the brain.
Now these impulses that are sent throughout the neurons are not as simple as singular electrical messages. These impulses are made by incredibly rapid depolarisation and repolarisation (basically a change in the electrical potential within the cell from negative to positive and then back again) of the membrane potential within the neuron which will make something called an action potential (AP). These APs can travel down their Axon at very fast speeds. Imagine this AP as an electrical message that just trundles (at break neck speed) down this road [7].
Another problem occurs when there is a gap between the two neurons (such as when the axon meets the adjacent neurons dendrites). This gap is called a synapse. The bodies way of solving this is by the use of Neurotransmitters (NT). These are chemicals that are released from the pre-synaptic neuron when the AP reaches the end of the neuron. These NTs (such as dopamine) then make their way across the synaptic ‘abyss’ where they attach to the post-synaptic neuron which in turn causes another action potential in the next neuron.
So, what is the point in this post? I suppose the main question I would like to explore is: Whether/ how cannabis should be used medically in our society (the UK specifically)? I am going to approach this from a medical perspective, because although there are other remits which one could explore, I am not hugely determined to pursue these branching avenues on the past uses, political aspects or the recreational uses. I would like to try and highlight the mechanisms of action that cannabis has, and how this may and has been used therapeutically.
As one of the most abused drugs in the world, and there seems to be an ever-growing inconsistency between the science behind cannabis and the myths. I feel there is a split between these pseudo-scientists who seem to think cannabis will be some sort of panacea for all earthly ailments and those who are so anti that they remain obstinate in the face of actual evidence.
The former claiming some senseless benefits such as ‘lighting up unlocks your creative potential and helps you lose weight’, whilst also failing to mention the myriad of downsides such as risk of psychosis, cardiovascular disease, infertility and general mental health problems. The latter giving either contradictory or irrelevant information (such as cannabis increases the risk of car accidents, I mean, so does a blindfold, just not sure how it is a downside just don’t drive).
At the end of the day there is probably valid points from both sides of this 10,000-year-old fence. And it undoubtedly comes down to type and moderation. I mean the risk to someone who makes their own hempseed milk and is “partial to some whacky-tobacco” is negligible in comparison to someone who smokes skunk daily.
Definitions
I think it would be useful to first separate some terms so that there can be no confusion. During the course of this blog Cannabis will be used to denote both Hemp and Marijuana, technically both of these substances are classed as cannabis, but their morphology, and chemical make-up are very different. Cannabis belongs to the family (Cannabaceae) that has just one genus (Cannabis), there are several species of cannabis from sativa to indica to ruderalis, the largest variety being cannabis sativa. It is a dioecious plant which means it can be separated into male and female plants, each with different properties[1]. Hemp is a variety of Cannabis sativa L and has a variety of uses from the fibre in the stems to make ropes (some hemp ropes have dated back to 26,900 BCE)[2], fabrics, paper and building materials. The seeds can be used as fuel or food and the leaves and flowers can be cultivated into CBD oil [3] Marijuana comes from the Indian Hemp seed and is cultivated purely for the intoxicating effects of its female flowers/buds. [4]
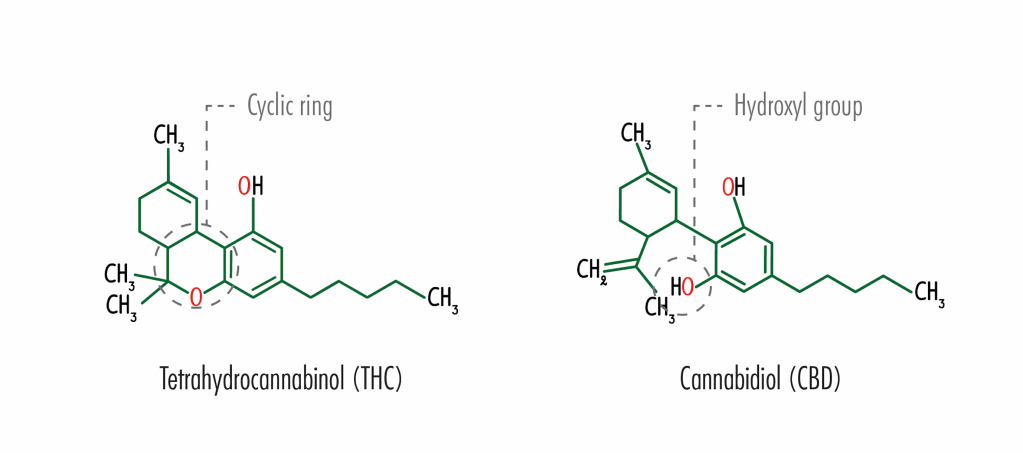
Tetrahydrocannabinol (THC) and Cannabidiol (CBD)
Structural formula of Tetrahydrocannabinol (THC) and Cannabidiol (CBD)
So where exactly does the intoxicating and therapeutic effect of these cannabis plants come from? These plants produce a huge array of phytochemicals (biologically active compounds in plants) including a broad range of cannabinoids, famously including tetrahydrocannabinol (THC) and cannabidiol (CBD). The notorious yin and yang of cannabis. There are actually over 60 different types of (Phyto)cannabinoids within cannabis with THC and CBD just being two of them [5]. These cannabinoids work in our body on something called the Endocannabinoid system (EC). The EC system is a molecular system that is responsible for regulating numerous processes within the body, these include the immune response, cellular communication, appetite, memory and many others. For something that has such a crucial role in the body, it is surprising to note that the EC system wasn’t discovered until ~ 30 years ago by a molecular biologist named Lisa Matsuda [6]. Before delving into the workings of the EC system it would be worth mentioning some knowledge of basic neurotransmission may be useful. (If you understand Action potentials, synapses and neurotransmitters then you can skip this bit then read on, if not here is a link to another blog that will explain it: (https://neuro7.home.blog/2020/06/04/the-basics-of-neurotransmission/)
The Endocannabinoid (EC) system
The EC system relies on 3 essential components: The endocannabinoids (the natural cannabinoids made by the body), The receptors (molecules that the endocannabinoids can bind to) and the enzymes (these break down the endocannabinoids once their role is complete). The EC systems communicates messages slightly differently because it does it ‘backwards’, so essentially when the post synaptic neuron is activated by the neurotransmitter it causes the creation of endocannabinoids (they are of Neurotransmitters for the EC system) that can then travel back toward the pre-synaptic neuron where they attach to cannabinoid receptors. This is important because they can act as a sort of dampener, controlling how much neurotransmitter (e.g. dopamine) can be released in future [7].
There are two main types of cannabinoid receptor (CB1 and CB2) that when bound to cause varying effects depending on where there are in the body and what endocannabinoid it is bound to. CB1 receptors are primarily found in the brain and central nervous system, these CB1 receptors seem to mediate many of the psychoactive effects of cannabinoids. The CB2 receptors are distributed throughout the immune system and peripheral nervous system and seem to be responsible for anti-inflammatory and other immune system responses [8]. It’s on the EC system that these Phyto-cannabinoids: THC and CBD play a role.
Mechanisms and therapeutic potential of THC
THC is a molecule that can mimic these endocannabinoids. When someone ingests THC, the body may be overrun with the substance thus interfering with the natural cannabinoid within the body. I have heard the clichéd line “we have marijuana receptors in our body” which isn’t strictly wrong but is rather misused. Instead it should be “we have receptors in our body that marijuana can bind to and mimic the effect of the natural endocannabinoid neurotransmitters”. THC can bind to both CB1 and CB2 very strongly and because these receptors are everywhere the overstimulation by THC causes such a wide variety of effects, some good some bad [9].
They are in the Amygdala which controls emotions such as fear and anxiety and thus overstimulation induces a paranoia effect. They are in the Basal ganglia which is an area of the brain which helps start our movement (over stimulation causes slowed reaction times). They are in the Hippocampus controlling memory formation (and thus forgetfulness) and the Hypothalamus controlling appetite (and thus the munchies). These are just some of the area that these CBs inhabit but we can already see how overstimulation by THC will cause problems all over the body and brain [10][11].
Diagram to show different brain regions that CB1 receptors are located in and the role that the brain region has.
THC is not all doom and gloom and there are potential treatments using THC due to the fact that it can bind to these CB receptors very strongly. It therefore can have many similar effects to the natural cannabinoids and also some of the effects that CBD can cause. It will act as a pain reliever, reducing nausea, anti-inflammatory and increasing appetite so there are definitely benefits to the use of THC. There are indeed approved medical treatments that use just THC such as oral THC (Marinol) that is approved for use in the US to treat nausea and vomiting due to chemotherapy; however, for me, what it comes down to is that everything THC can do, CBD can do it better and with fewer side effects. In fact, the only areas where THC seems to blaze a trail is in its ability to induce a “high” and also increase appetite.
Mechanisms and therapeutic potential of CBD
That’s THC, but what about CBD – this apparent panacea. One of the key differences between the effects of both these substances is that CBD doesn’t have the intoxicating effects that THC has this is because it is not psychotropic and doesn’t strongly bind to these CB receptors mentioned above. There are various ideas as to how CBD actually acts on the body, with some suggesting it works by preventing the breakdown of the (natural) endocannabinoids thus causing them to have a longer lasting effect on the body. Studies have also shown that CBD can also bind to a variety of other receptors such as 5HT (Serotonin Receptors), TRPV, GPR55 and can also change the shape of the CB1 receptor preventing THC from binding directly to it [11].
Regardless of what exactly it binds to, CBD can bind to a lot of receptors, great! But what does this mean therapeutically? after all that’s what this comes down to. Is there a viable purpose other than as a recreational drug, to which a resounding answer would probably be: Yes.
5HT: For instance, by binding to 5HT, CBD may have a useful role in treating many disorders (such as depression and psychosis). This family of serotonin receptors are found throughout the nervous system. Tangentially when studying these topics, I am always astounded by the sheer multitude of effects that a single family of receptor can have in the body. Serotonin is no different and is said to influence various processes such as aggression, anxiety, appetite, cognition, learning, memory, mood, nausea, sleep and many others. I mean leave something for the other receptors. It is therefore purported that CBD can cause some antidepressant effects by binding to this 5HT receptor [12] .
There is also evidence proposing CBD as a treatment for psychosis as research has shown that the EC system itself may be involved in psychosis (with psychosis patients showing a higher level of the endocannabinoid (anandamide) and increased CB1 receptors) It is hoped CBD may effectively act as an act as an atypical antipsychotic, without the undesirable side effects which are often seen from other antipsychotics (what are termed extrapyramidal side effects (EPS))(some examples of other atypical drugs are clozapine and risperidone) [13][14]. The evidence at this point is reasonably sparse, with the need for more high-quality randomised control trials. There has been a couple of good quality trails (such as by McGuire et all in 2018) which have shown CBD to cause a slight improvement of positive symptoms of psychosis (these symptoms such as hallucinations and delusions) while also showing an improvement in the patient’s cognition and the impact of the illness on their day-to day lives. Further studies using patients suffering from psychosis (rather than animals or healthy participants) will allow for a wider array of concrete evidence. Finally, there is also evidence that suggests CBD provides an anti-emetic (anti-sickness) effect by indirect activation of a specific 5HT receptors in an area of the brain called the dorsal raphe nucleus [15]. The activation is therefore useful as a treatment for nausea caused by chemotherapy (in reality in a direct comparison between THC and CBD for treating nausea THC seems to perform better, in this case it may be a combination of both that proves most effective.)
TPRV1: CBD can also binds to this TPRV1 (Transient Receptor Potential Vanilloid Type 1), which is linked to the immune function and inflammation, pain, and control in the hypothalamus [16]. This will lead to some supposed analgesic (pain relief) effects of CBD, more specifically it has been shown to be an effective anti-hyperalgesic (hyperalgesia is an abnormal increased sensitivity to pain) for acute inflammation and chronic pain. Generally it seems CBD has promising effectiveness as an anti-inflammatory agent for nervous tissue inflammation, arthritis, IBD (Inflammatory Bowel Disease) and potentially certain types of cancer that are linked to chronic inflammation[17][18].
Epilepsy: Finally, CBD has some very proven effectiveness on Epilepsy. This is one of the most common serious neurological condition, with about 1 in 100 people having active epilepsy and ~ 1 in 50 people who will develop epilepsy during their life [19].
It is a group of disorders characterised by abnormal electrical activity in the brain, leading to unprovoked seizures. Epilepsy is a disorder which has no single diagnostic test that gives a definitive yes or no. There is not a single drug or treatment that is effective as a cure, the general consensus for drug treatment with epilepsy is to “start low – go slow”, where the goal is to find an effective treatment with the lowest drug treatment or combination that works.
(There are ~25 drugs that can be used to treat epilepsy as a monotherapy, when this doesn’t work as a treatment duo-therapy can be used (two drug therapy) leading to ~ 300 different drug combinations that may be effective. If the duo-therapy is not effective, then 3-drug treatment options can be used with about 2300 different combinations).
Even after all this, the treatment will only be effective in about 70% of cases, not to mention the fact that some of these drug treatments have some pretty dire side effects (such as Valproate, which can cause stomach upset, hair loss, tremor, bruising, and damage to an unborn child). What this really comes down to is that there are still ~30% of epilepsy cases that are untreatable by AEDs (Antiepileptic drugs) [20]. This is where treatment a substance such as CBD may be particularly useful. Dravets syndrome is a serious epilepsy that manifests in the first year of life and often lead to future difficulties such as poor language development, poor motor skills and development of chronic illness. There is also 20% mortality by age 20. It is also an epilepsy that is particularly resistant to AEDs.
This is one of the disorders where the use of CBD has been authorized as a potential treatment. There is evidence to show that CBD can half the the number of monthly seizures. This may be because CBD is able to inhibit receptors in the body (such as FABPs (a fatty acid binding protein) and the GPR55 mentioned earlier) that other AEDs don’t interact with [21][22] thus causing the natural endocannabinoids like anandamide to have a longer lasting effect in the body
Conclusion
Initially returning to the original question of “Whether / how cannabis should be used medically in the UK?” to be blunt: Yes. Obviously not for every known ailment, but there is undoubtedly evidence for cannabis (Either CBD or THC) being a valuable therapeutic tool across a wide range of conditions. The fact that we have a substance that can treat symptoms of nausea, anxiety, depression and appetite, while also being able to improve outcomes on debilitating diseases such as Epilepsy, psychosis and multiple sclerosis must give it some position to be credited as a valuable instrument in a health care professionals (HCPs) tool kit.
I think it partially comes down to is how we view and use these substances. Cannabis was classified as a Class B drug alongside its undoubtedly more dangerous counterparts such as Amphetamines and Ketamine – which can only be administered in a medical setting by trained professionals (and on the occasional horse). Up until 2018 cannabis was classified as having no redeeming value to society and in 2018 the legalisation of medical cannabis seemed like a step in the right direction to embrace its potential. Yet, it seems the British medical establishments remain decidedly unconvinced. A year later it seemed only ~20 NHS prescriptions had been issued (Mostly to infants with lethal epilepsy such as Dravets) [23].
This is probably due to the lack of acceptance from the medical community and also the extremely restrictive criteria laid for patient access. These misconceptions about the whole family of cannabis has created a sort of anti-cannabis hysteria with the only way to change being with real life data. There are of-course good steps being made in this area from numerous published and on-going studies as well as the massive increase in sales of CBD based products in the British retail markets, but there is definitely still a way to go.
Now coming to how it should be used, this poses a slightly more difficult question. For me the answer seems to be in the use of predominantly CBD based products with an aim to have greater regulation over the amount of THC. I don’t think anyone is really expecting a complete legalisation of cannabis both recreationally and medically because in all honesty that’s not beneficial. This country already has an alcohol problem, giving them another recreational drug probably isn’t going to help, possibly the only benefit would be a decrease in the number of street fights outside spoons. What is needed is clearer guidelines for HCPs on the appropriate use of cannabis in the most appropriate form, presumably something like oral CBD, or prescription medication with a low dose of THC. At the end of the day we can always see if Canada has space for us.
[5] Z. Atakan, ‘Cannabis, a complex plant: Different compounds and different effects on individuals’, Therapeutic Advances in Psychopharmacology, vol. 2, no. 6. SAGE Publications, pp. 241–254, 2012.
[7] P. Pacher, S. Bátkai, and G. Kunos, ‘The endocannabinoid system as an emerging target of pharmacotherapy’, Pharmacological Reviews, vol. 58, no. 3. NIH Public Access, pp. 389–462, 2006.
[8] S. Zou and U. Kumar, ‘Cannabinoid receptors and the endocannabinoid system: Signaling and function in the central nervous system’, International Journal of Molecular Sciences, vol. 19, no. 3. MDPI AG, 13-Mar-2018.
[9] B. E. Alger, ‘Getting high on the endocannabinoid system.’, Cerebrum, vol. 2013, p. 14, Nov. 2013.
[11] D. A. Kendall and G. A. Yudowski, ‘Cannabinoid receptors in the central nervous system: Their signaling and roles in disease’, Front. Cell. Neurosci., vol. 10, p. 294, Jan. 2017.
[12] E. B. Russo, A. Burnett, B. Hall, and K. K. Parker, ‘Agonistic properties of cannabidiol at 5-HT1a receptors’, Neurochem. Res., vol. 30, no. 8, pp. 1037–1043, Aug. 2005.
[13] J. Renard, C. Norris, W. Rushlow, and S. R. Laviolette, ‘Neuronal and molecular effects of cannabidiol on the mesolimbic dopamine system: Implications for novel schizophrenia treatments’, Neuroscience and Biobehavioral Reviews, vol. 75. Elsevier Ltd, pp. 157–165, 01-Apr-2017.
[14] A. Waldo Zuardi et al., ‘A Critical Review of the Antipsychotic Effects of Cannabidiol: 30 Years of a Translational Investigation’, Curr. Pharm. Des., vol. 18, no. 32, pp. 5131–5140, Sep. 2012.
[15] L. A. Parker, E. M. Rock, and C. L. Limebeer, ‘Regulation of nausea and vomiting by cannabinoids’, Br. J. Pharmacol., vol. 163, no. 7, p. 1411, 2011.
[16] T. Lowin and R. H. Straub, ‘Cannabinoid-based drugs targeting CB1 and TRPV1, the sympathetic nervous system, and arthritis’, Arthritis Research and Therapy, vol. 17, no. 1. BioMed Central Ltd., 06-Sep-2015.
[17] J. M. Nichols and B. L. F. Kaplan, ‘Immune Responses Regulated by Cannabidiol’, Cannabis Cannabinoid Res., vol. 5, no. 1, pp. 12–31, Mar. 2020.
[18] F. Afrin et al., ‘Can hemp help? Low-THC cannabis and non-THC cannabinoids for the treatment of cancer’, Cancers, vol. 12, no. 4. MDPI AG, 01-Apr-2020.
[20] M. M. Goldenberg, ‘Overview of drugs used for epilepsy and seizures: Etiology, diagnosis, and treatment’, P T, vol. 35, no. 7, pp. 392–415, Jul. 2010.
[21] R. Mechoulam, ‘Cannabis and epilepsy’, Epilepsy and Behavior, vol. 70. Academic Press Inc., pp. 278–279, 01-May-2017.
[22] E. B. Russo, ‘Cannabis and epilepsy: An ancient treatment returns to the fore’, Epilepsy and Behavior, vol. 70. Academic Press Inc., pp. 292–297, 01-May-2017.
I would like to start this journey into reality with the idea of consciousness; it’s a word thats used a lot and seems to have a number of meanings, but on this blog I am going to classify it into two parts: one is our experiences of the world around us and all that we can perceive. It is our ability to orient and appreciate the external world through our sacks of blood, organs and brain. The second is our conscious-self; this is what separates me from you and gives us our feeling of self-identity. In this post, I am going to particularly draw attention to the idea of consciousness in the world around us.
It is often assumed that our senses allow us to perceive the world as it actually is, this so-called reality that we choose to bob around in. What it actually comes down to is whether our brains are able to accurately interpret the multitude of inputs it receives all the time. Our brains do not really know what is out there in the world. It does not see light or listen to sounds it merely receives electrical impulses that let it have a good guess at what is going on. What we are perceiving (or perhaps more accurately hallucinating) is just our brains’ interpretation. So how do we know what we hallucinate is correct? Well we don’t; however, when our ‘hallucination’ matches what others say they are perceiving then that’s what we call reality. Most of the time this reality is consistent for everyone, but sometimes these processes can create different outcomes for different people causing us to perceive different things.
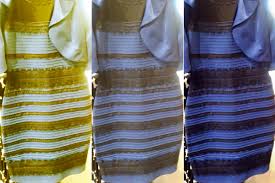
A good example of this is that white/black dress debacle from a few years ago. This particular illusion comes from the idea that we have evolved to see in daylight, which has a range of colours from pinkish-red to blue-white. Now when our brain perceives inputs in the visual cortex it is programmed to subtract the information about the illuminant (that is the wavelengths of light illuminating the world and bouncing off the object) and to find information on the actual reflectance (the proportion of light that is reflected when striking the object). Because daylight has such a wide spectrum of colour the brain may subtract either the blueish colour and thus leave the dress looking white/gold or will subtract the gold-side therefore leaving the dress looking blue/black.
I think it may be best to limit this post to just the processes of visual perception; of course there are whole other systems of auditory and tactile perception that also interpret the world through the inputs they receive, but I think it’s easier to picture the visual process.
So how do we perceive the world? One might assume that the eyes just take perfect snapshots of the world and relay them to the visual cortex where we browse through this chronological slideshow of our lives. In reality our eyes just perceive a sort of 2D shadow world, from which our brain makes predictions on what/where everything is. When we look at the world around us, we absorb spatial patterns of light that bounce off different objects and land on the flat surface of our eye. This two-dimensional map is then sent to the brain where it must construct a three-dimensional image of the world. The problem with this is that many different objects can all cast the same shadow so knowing which one is correct is sometimes a difficultly. There is also the issue that the brain doesn’t have hours to ponder this, it has a fraction of a second. When a ball is thrown at your face there is a rapid and continuous flow of information that has to dealt with, which will be the decider between some safe hands or some broken teeth.
The brain has to deal with these challenges, being constantly bombarded with this plethora of information. It has to be able to process it efficiently to generate an accurate picture of the world. A way it optimises this process is to try and predict what sensory inputs we will receive based on what we have experienced before. We do not simply rely on the input coming into the sensory receptors instead these inputs are combined with our expectations about what we should be perceiving. This is because it is far less strenuous for the brain to create an improvised reality based on educated guesses and using a few simple rules or assumptions.
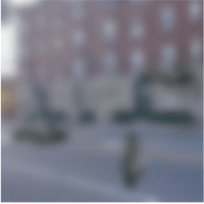
If you look at the picture, you may be able to make out a street with a car driving along and a pedestrian on the pavement. In actual fact both the car and the pedestrian are the same image, but the pedestrian image is rotated and made smaller. The fact that we see this street as a car and a pedestrian is due to the fact that the visual input is weak or ambiguous and therefore the brain is more likely to rely on prior expectations. The shapes themselves show no information to define them as either car nor object, but the context of the street leads us to perceive them this way.
This idea of prior expectation really affects how we perceive our world and is likely acquired over a lifetime of experience. This theory is an incarnation of the “Bayesian Brain” which proposes this kind of probabilistic inference occurs when our sensory signals (Bottom-up processing) is assessed with our prior knowledge (Top-down processing) about a situation. This model of Bayesian inference uses the method of predictive coding which uses prediction errors to minimise the amount of sensory information the brain receives. A prediction error is the difference between the actual and expected incoming information and can be transmitted to the brain to improve efficiency of signal transmission.
In terms of the actual neurological structures behind how these processes work, fMRI have shown that there may be a feedback from higher to lower level sensory cortices. This feedback is assumed to be these prediction errors and have shown that some neural responses are dampened when the predictions made are confirmed by the input from the sensory systems. These signals are enhanced when the prediction does not match. For example, when you are bothered by a constant sound, such as someone chewing loudly or the incessant whirring of an air-conditioning unit, the noise will at first be distracting. It will bore into your brain leaving you unable to focus on the most basic task until at some point, it will cease to be distracting. This is because the brain is able to predict the sound and dampen it; however, when the noise stops that silence will hang in the air and will be very noticeable for the same reason that our brain expects to be ‘hearing’ it. Another example is why we find it very difficult to tickle our self. The brain can predict the sensory effect of the movement and dull this stimuli.
I feel as though this point of how our expectations shape our reality has been laboured enough by me, so to conclude this post I think it comes down to how we view this term hallucination. If it is a perception of something not present then where do we draw this line between what is present and what we expect to be present? The fact that we can perceive the world through this anticipatory, pre-activated brain, where our expectations seem to drive our reality begs the question of how much is misrepresented in the world around us, and how much of our perception is down to our inherent beliefs about the world?